Borderline Ovarian Tumors: Definition, Diagnosis and Treatment
What is a Borderline Ovarian Tumor?
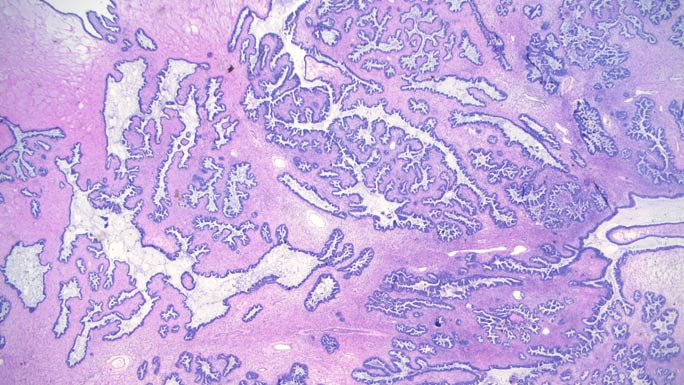
Borderline ovarian tumors, often referred to as “low malignant potential” tumors, are not invasive but also not completely benign. Their behavior can also vary based on microscopic features, and some are more likely to recur or spread than others.
Types of Borderline Ovarian Tumors
At the University of Chicago Medicine, our specialists treat all types of borderline ovarian tumors, including:
- Serous, the most common type, which start in the surface of the ovary and often affect younger women; they are filled with fluid and often found in both ovaries
- Mucinous, the second most common type, which are filled with mucus-like fluid; they usually affect only one ovary
- Endometrioid, a rare tumor with cells similar to those lining the uterus (endometrium) and is often linked to endometriosis
- Clear cell, a very rare tumor made of clear cells
- Seromucinous, another very rare tumor that shares features with serous and mucinous tumors
- Borderline Brenner tumors, extremely rare tumors that form in the tissue covering the ovary
Symptoms of Borderline Ovarian Tumors
Signs of borderline ovarian tumors include:
- Pain or pressure in the pelvis or abdomen
- Swelling in the stomach area or abdomen
- Vaginal bleeding unrelated to menstrual cycle
- Pain during or after intercourse
- Feeling full soon after eating
- Constipation or more frequent bowel movements
- Needing to urinate more frequently
Borderline Ovarian Tumor Diagnosis
Your doctor may diagnose you with a borderline ovarian tumor based on several tests, including:
- Pelvic exam: To feel your ovaries, your provider will insert a finger inside your vagina and press down gently on your abdomen.
- Transvaginal ultrasound: During this procedure, your provider will insert an ultrasound wand into your vagina. The wand uses sound waves to detect tumors in the ovaries.
- Magnetic resonance imaging (MRI) scan: This advanced imaging test provides detailed pictures of your ovaries and helps doctors determine if a tumor is benign, malignant or borderline.
- Biopsy: A biopsy is the primary method to diagnose a borderline ovarian tumor. Most biopsies for borderline ovarian tumors are performed during surgery. Our pathologists examine biopsied tumor cells under high-resolution microscopes to determine the correct diagnosis, which will then guide treatment.
If you have been diagnosed with a borderline ovarian tumor, our gynecologic oncologists can support you.
Find an Ovarian Tumor Specialist
Borderline Ovarian Tumor Treatment
For nearly all borderline tumors, surgery is the only treatment needed – even when borderline tumors have spread to other areas. Surgery may involve removing the mass alone or the affected ovary and fallopian tube. In some situations, endocrine (hormone) therapy after surgery may be considered.
In young patients, fertility-sparing surgery or preservation of an unaffected ovary to avoid surgical menopause is often possible. Surgical menopause refers to menopause that is caused by the surgical removal of the ovaries, as compared to menopause that occurs as part of the natural aging process. Learn more about fertility services for cancer patients.
Our team of gynecologic cancer specialists will discuss in detail the extent of surgery that is indicated based on your specific needs. Whenever possible, we use minimally invasive (laparoscopic) surgery that is performed through smaller incisions. This approach typically results in a faster recovery, minimal scarring and a reduced risk for post-surgical complications as compared to a traditional open surgical procedure. Tissue removed during surgery will be reviewed by our expert gynecologic pathologists to confirm an accurate diagnosis. Information from the pathologist’s report will guide an individualized follow-up plan that is tailored to your needs.
Surveillance After Treatment
Patients with borderline ovarian tumors will need to continue long-term follow-up care. In women who still have one ovary after their initial surgery, periodic imaging with ultrasound may be recommended. Although the risk of recurrence is low overall, some borderline tumors can recur several years after initial diagnosis.
It is rare, but borderline tumors can recur as slow-growing, low-grade cancers that require more aggressive treatment. Our team will provide you with a detailed plan for your follow-up surveillance care. For patients who do not live close to UChicago Medicine, this plan frequently includes your general gynecologist closer to home to ensure safe and convenient follow-up care.
Treatment for Recurrent Borderline Ovarian Tumors
Approximately 10% of borderline tumors may recur either as borderline tumors or as invasive cancers. Recurrences are typically treated surgically, both to ensure there is not a low-grade cancer component and because borderline tumors often do not respond well to systemic treatments such as chemotherapy. Our gynecologic cancer surgeons use minimally invasive (laparoscopic) techniques for recurrences whenever possible, depending on the location of the tumor.
When needed, our highly skilled team of surgeons also excels at performing complex debulking surgeries to remove as much tumor as possible, which is similar to the treatment approach for advanced ovarian cancer. With appropriate surgery, many patients will experience a long remission. In many instances, we consider doing surgery at the time of a second or later recurrence. Our team of experts is highly experienced in managing ovarian masses, including borderline tumors, and will work with you to find the right approach to ensure the best possible outcome.
Convenient Locations for Gynecologic Oncology Care
Request an Appointment
We are currently experiencing a high volume of inquiries, leading to delayed response times. For faster assistance, please call 1-855-702-8222 to schedule your appointment.
If you have symptoms of an urgent nature, please call your doctor or go to the emergency room immediately.
* Indicates required field
Cancer Care Second Opinions
Request a second opinion from UChicago Medicine experts in cancer care.

Participate in a Clinical Trial
UChicago Medicine ovarian cancer experts are actively conducting clinical trials of new and promising treatments.

Gynecologic Cancer Prevention Clinic
Our cancer prevention experts provide comprehensive and personalized care for women at elevated risk for endometrial (uterine) cancer and ovarian cancer.