HPV-Related Head and Neck Cancer Treatment
Less Intense Treatment Strategy Cures Many HPV-related Cancers
Almost 80 million people have been infected with human papillomavirus (HPV), which is now the most common sexually transmitted infection in the United States. Most people are able to clear the HPV virus without being treated, but those who can’t are at increased risk for developing cancer in the tonsils and base of the tongue.
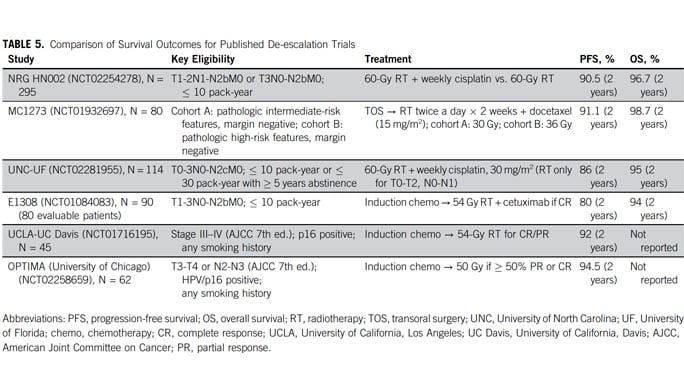
Aggressive treatments developed for tobacco-related head and neck cancers over-treat most patients with HPV-related cancer. A new, less intense strategy is curing many of these patients while preserving their ability to swallow, speak and eat. Our approach resulted in the nation's leading survival rate for HPV-related cancers: ~95% of our patients were still alive after two years, and patients treated with reduced radiation were less likely to need feeding tubes.
Medical oncologist Alexander Pearson, MD, PhD, co-director of the head and neck cancer program at the University of Chicago Medicine, discusses HPV-linked head and neck cancer and new treatments for the disease.
Less Invasive Treatment Effective for HPV-Linked Head and Neck Cancer

Request an Appointment
We are currently experiencing a high volume of inquiries, leading to delayed response times. For faster assistance, please call 1-855-702-8222 to schedule your appointment.
If you have symptoms of an urgent nature, please call your doctor or go to the emergency room immediately.
For Referring Physicians
To refer a patient for head and neck cancer care, please call UCM Physician Connect at 1-800-824-2282.
* Indicates required field

Cancer Care Second Opinions
Request a second opinion from UChicago Medicine experts in head and neck cancer care.

Participate in a Clinical Trial
UChicago Medicine head & neck cancer experts are actively conducting clinical trials of new and promising treatments.

Helping You Cope With Cancer
Our Supportive Oncology program offers a range of services to support you and your family during your cancer treatment.
Head & Neck Cancer: Q & A

Head & Neck Cancer: Q & A
Medical oncologist Alexander T. Pearson, MD, PhD, and nurse navigator Patricia Heinlen, BSN, RN, discuss head and neck cancer, including the HPV vaccine and how new treatment approaches are tailored to each patient's cancer type, making treatments more effective while reducing side effects.